Study Finds Little to No Cortical Lewy Pathology in Living Parkinson’s Disease Patients Undergoing Deep Brain Stimulation
Findings challenge longstanding assumptions about how disease progresses and may redefine understanding of subtypes
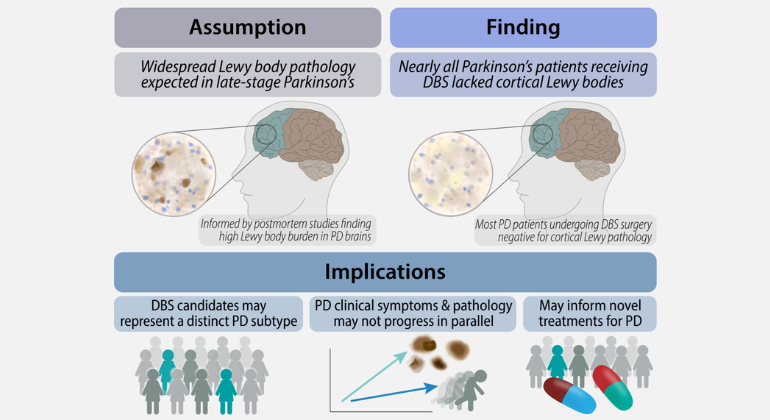
Credit: Ariela Buxbaum Grice, graduate student at the Icahn School of Medicine at Mount Sinai and lead author of the study.
Researchers at the Icahn School of Medicine at Mount Sinai have found that patients with Parkinson’s disease undergoing deep brain stimulation (DBS) show little to no Lewy pathology in the prefrontal cortex at the time of their DBS surgery, despite often having longstanding, clinically advanced disease.
Published in NPJ Parkinson’s Disease [DOI: https://doi.org/10.1038/s41531-026-01422-8], the findings provide important new insight into the relationship between Parkinson’s disease clinical symptoms and neuropathological progression.
Lewy bodies are abnormal clumps/aggregates of the protein alpha-synuclein that build up inside nerve cells in the brain and are considered a pathological hallmark of Parkinson's disease and are believed to accumulate throughout the brain as the disease progresses. The absence of this pathology, particularly among patients presumed to be in later stages of disease progression, was therefore unexpected. Previous studies—largely in postmortem tissue—have consistently found widespread Lewy pathology in patients with advanced Parkinson’s disease. However, little was previously known about how this hallmark of disease appears in individuals, especially at the time of DBS surgery.
As part of Mount Sinai’s Living Brain Project, researchers analyzed prefrontal cortex samples taken during deep brain stimulation procedures in patients with Parkinson’s disease and in patients undergoing DBS for other neurologic conditions. Researchers then compared the tissue samples to determine whether patients with Parkinson’s disease had a greater burden of cortical Lewy pathology than the comparison group.
Unexpectedly, nearly all biopsies from patients with Parkinson’s disease undergoing DBS were negative for Lewy bodies, and the overwhelming majority also lacked Lewy neurites, the abnormal nerve-cell proteins associated with Lewy pathology. In contrast, matched postmortem samples from individuals with Parkinson’s disease showed, as expected, a higher burden of Lewy pathology than control samples.
“We were surprised to find that almost none of the patients living with Parkinson’s disease had cortical Lewy bodies, particularly because many had been living with the disease for years,” said Ariela Buxbaum Grice, a graduate student at the Icahn School of Medicine at Mount Sinai and lead author of the study. “Because this finding was so unexpected, we carefully evaluated the most likely technical explanations and found that none could explain the near-absence of Lewy bodies. That gives us confidence that this reflects a true biological characteristic within this patient population, as opposed to a laboratory artifact.”
Noam D. Beckmann, PhD, Assistant Professor of Artificial Intelligence and Human Health at the Icahn School of Medicine at Mount Sinai and senior author of the study, said the findings underscore the importance of studying molecular pathology in the context of clinical characteristics.
“This study demonstrates that clinical severity, disease progression, and neuropathological burden do not always advance together,” Dr. Beckmann said. “By studying living brain tissue alongside detailed clinical data, we can begin to identify biologically meaningful subtypes of Parkinson’s disease and better understand how the disease progresses, helping to guide more personalized treatment strategies in the future.”
The study also highlights the value of the Living Brain Project, a multiscale, data-driven research initiative that enables researchers to study living brain tissue collected during neurosurgical procedures. By integrating neuropathological analysis with detailed clinical information, investigators can better understand disease biology as it develops in living patients, rather than relying solely on tissue collected after death.
Brian Kopell, MD, Director of the Center for Neuromodulation, Co-Director of The Mount Sinai Hospital Movement Disorders Program, and Co-Lead of the Living Brain Project, emphasized the importance of studying living brain tissue in patients during advanced neurosurgical treatment.
“Deep brain stimulation offers a rare opportunity to study the biology of Parkinson’s disease directly in living patients,” Dr. Kopell said. “Many of the patients had clinically significant motor symptoms but showed very limited cortical Lewy pathology. That disconnect could change how we think about disease progression and which patients may benefit most from deep brain stimulation.”
Alexander Charney, MD, PhD, Director of The Charles Bronfman Institute for Personalized Medicine; Professor of Psychiatry, Neuroscience, and Genetics and Genomic Sciences at the Icahn School of Medicine at Mount Sinai; Co-Lead of the Living Brain Project; and co-senior author on this manuscript, said the findings suggest that DBS candidates may represent a biologically distinct subgroup of Parkinson’s disease patients.
“These findings challenge the assumption that patients undergoing deep brain stimulation necessarily have widespread cortical Lewy pathology based solely on disease duration or symptom severity,” Dr. Charney said. “Instead, our findings suggest that many DBS patients may represent a motor-predominant subtype of Parkinson’s disease with relatively limited cortical involvement.”
The findings suggest that Parkinson’s disease may progress differently across biologically distinct patient groups, highlighting the complexity of the disease and the need for additional research. Rather than reflecting uniformly advanced neuropathology, patients selected for deep brain stimulation may represent a subgroup with slower or regionally distinct patterns of Lewy body accumulation.
Additional longitudinal and postmortem studies will be needed to determine whether DBS patients experience slower cortical disease progression or represent a distinct biological subtype of Parkinson’s disease.
This work was supported by the National Institute on Aging and the Michael J. Fox Foundation.
About the Icahn School of Medicine at Mount Sinai
The Icahn School of Medicine at Mount Sinai is internationally renowned for its outstanding research, educational, and clinical care programs. It is the sole academic partner for the seven member hospitals* of the Mount Sinai Health System, one of the largest academic health systems in the United States, providing care to New York City’s large and diverse patient population.
The Icahn School of Medicine at Mount Sinai offers highly competitive MD, PhD, MD-PhD, and master’s degree programs, with enrollment of more than 1,200 students. It has the largest graduate medical education program in the country, with more than 2,700 clinical residents and fellows training throughout the Health System. The Graduate School of Biomedical Sciences offers 12 degree-granting programs, conducts innovative basic and translational research, and trains more than 470 postdoctoral research fellows.
Ranked 11th nationwide in National Institutes of Health (NIH) funding, the Icahn School of Medicine at Mount Sinai is among the 90th percentile of U.S. private medical schools in Sponsored Programs Direct Expenditures per Principal Investigator, according to the Association of American Medical Colleges. More than 6,900 scientists, educators, and clinicians work within and across dozens of academic departments and multidisciplinary institutes with an emphasis on translational research and therapeutics. Through Mount Sinai Innovation Partners (MSIP), the Health System facilitates the real-world application and commercialization of medical breakthroughs made at Mount Sinai.
-------------------------------------------------------
* Mount Sinai Health System member hospitals: The Mount Sinai Hospital; Mount Sinai Brooklyn; Mount Sinai Morningside; Mount Sinai Queens; Mount Sinai South Nassau; Mount Sinai West; and New York Eye and Ear Infirmary of Mount Sinai
About the Mount Sinai Health System
Mount Sinai Health System is one of the largest academic medical systems in the New York metro area, with approximately 48,000 employees working across seven hospitals, more than 400 outpatient practices, more than 600 research and clinical labs, a school of nursing, and leading schools of medicine and graduate education. Mount Sinai advances health for all people, everywhere, by taking on the most complex health care challenges of our time—discovering and applying new scientific learning and knowledge; developing safer, more effective treatments; educating the next generation of medical leaders and innovators; and supporting local communities by delivering high-quality care to all who need it.
Through the integration of its hospitals, labs, and schools, Mount Sinai offers comprehensive health care from conception through geriatrics, leveraging innovative approaches such as artificial intelligence and informatics while keeping patients’ medical and emotional needs at the center of all treatment. The Health System includes more than 9,000 primary and specialty care physicians and 10 free-standing joint-venture centers throughout the five boroughs of New York City, Westchester, Long Island, and Florida. Hospitals within the System are consistently ranked by Newsweek’s® “The World’s Best Smart Hospitals,” “Best in State Hospitals,” “World’s Best Hospitals,” and “Best Specialty Hospitals” and by U.S. News & World Report's® “Best Hospitals” and “Best Children’s Hospitals.” The Mount Sinai Hospital is on the U.S. News & World Report® “Best Hospitals” Honor Roll for 2025-2026.
For more information, visit https://www.mountsinai.org or find Mount Sinai on Facebook, Instagram, LinkedIn, X, and YouTube. To listen to news and stories from Mount Sinai, visit the Mount Sinai Podcast Network.