
Acoustic Neuroma/Vestibular Schwannoma
Mount Sinai is a global leader in the treatment of acoustic neuroma/vestibular schwannoma, which is a benign tumor of the eighth cranial nerve that can cause hearing loss, tinnitus, and vertigo. In addition to standard approaches, our surgeons are trailblazers in using new and advanced technology to perform minimally invasive surgery. We routinely use endoscopes and high-resolution robotic microscopes, called ‘exoscopes,’ to gain access to difficult-to-reach areas to avoid larger operations with more morbidity.
About Acoustic Neuroma/Vestibular Schwannoma
Acoustic neuromas (vestibular schwannomas) are uncommon, benign tumors of the hearing and balance nerve that often cause progressive hearing loss in one ear. They are among the most common brain tumors; however, they occur in only 2-4 of every 100,000 people. This translates to approximately 6,000-8,000 new acoustic neuromas diagnosed in the United States each year.
Symptoms and Diagnosis of Acoustic Neuroma
In many cases of acoustic neuroma, the chief complaint is hearing loss in one ear. Hearing loss tends to progress gradually, although sudden hearing loss is possible. Patients may also experience impaired auditory processing from the side of the tumor even with minor hearing loss. Additional common symptoms include tinnitus (ringing in the ear), vertigo, and imbalance.
Not every patient with an acoustic neuroma has hearing loss, though. Some people maintain normal hearing even with large tumors. Hearing loss does not always correlate to tumor size.
In larger tumors, other symptoms of an acoustic neuroma may include:
- Facial twitching
- Headache
- Facial numbness or tingling
- Drowsiness and possible loss of consciousness
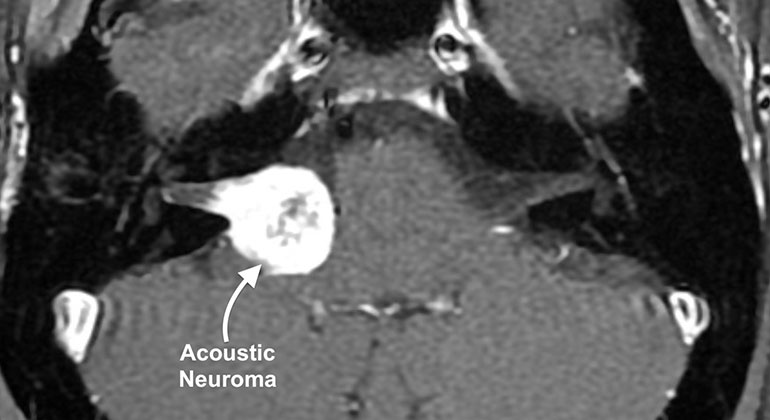
Acoustic neuromas are typically discovered after an abnormal hearing test (audiogram) that prompts an MRI demonstrating a tumor. We measure the tumor in 3 dimensions and compare each dimension and overall volume to assess growth over time.
Treatments for Acoustic Neuroma at Mount Sinai
A personalized treatment plan is developed for each patient. The selection of treatment depends upon several factors:
- Size of the tumor and whether it is compressing vital structures
- Symptoms and their duration
- Patient’s age
- Other medical issues
Patients with newly discovered acoustic neuromas receive full consultation with members of our multidisciplinary skull base surgery team and includes an examination of hearing and balance, as well as the surrounding cranial nerves. Results of the relevant scans and tests will be discussed at those visits, and we often discuss the cases as a tumor board (group) setting.
The treatment options for acoustic neuroma include:
- Surgical Resection: This is the only treatment option with the possibility of cure. During surgery, monitoring and preserving the nerves that control facial movement and hearing (in those that still have good hearing) are the top priorities. While we always attempt to remove the entire tumor, we may leave a very small piece intentionally to prevent facial paralysis or total hearing loss. With continuous monitoring and specialized dissection instruments, we are able to achieve excellent facial nerve and hearing preservation outcomes. Even in cases in which a small piece of tumor is left inside, the chance of this growing in a meaningful way is quite low. Our surgical team is highly skilled in all approaches, including retrosigmoid, translabyrinthine, and middle fossa. In very specific cases, we endoscopically remove the entire tumor through the ear canal using a small camera.
Decisions regarding surgical approach are largely a technical matter, and each option achieves excellent results in appropriately selected patients. Our philosophy is to select the best approach for each individual and our shared priorities. - Serial observation: Because acoustic neuromas are usually slow growing tumors, we often recommend monitoring the tumor at regular intervals for signs of growth if there is no compelling reason to operate immediately. For example, in older patients, if the tumor is small, it may never reach a size where it becomes life threatening. Hence, simple observation may be all the treatment that is needed. In properly selected patients, approximately 50 percent of tumors may remain stable in size and avoid the need for active treatment.
- Stereotactic radiation: Acoustic neuromas can be treated by a specialized form of radiation, called stereotactic radiotherapy (“radiosurgery”). This treatment delivers a high dose of radiation to the tumor while avoiding collateral damage to the sensitive surrounding brain, nerves, and bone. In properly selected patients, radiotherapy is effective in freezing tumor growth with rapid recovery and return to work. Radiation treatment may not be appropriate for large tumors that press on the brain. In these cases we typically recommend surgical resection.
A Comparison of Surgery versus Stereotactic Radiation
|
Microsurgery |
Stereotactic Radiation
|
|
Tumor removed completely |
Tumor still present, but usually freezes growth. |
|
Long-term cure in most, re-growth uncommon |
Re-growth can occur; long-term results uncertain |
|
Hospitalization |
No hospitalization |
|
Facial nerve weakness can occur |
Facial nerve weakness uncommon, usually temporary |
|
Hearing loss may occur, but hearing preservation possible in select cases |
Hearing often declines within a few years after treatment |
|
Dizziness common in the beginning but improves over time. |
Dizziness may remain stable or worsen. |